Long Thoracic Nerve/Serratus Anterior Palsy
What is it?
Pain referral pattern:
Diagnostic tool to rule in/out:
What is it?
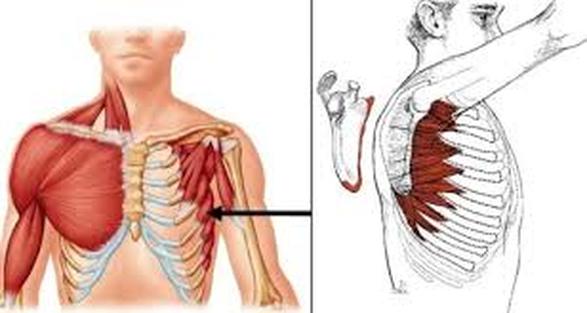
- An injury to the long thoracic nerve, which reduces the use of the serratus anterior muscle
- Anatomical considerations
- The only nerve to innervate serratus anterior, which means that any damage is detrimental
- Stems from the ventral rami of the 5th, 6th and 7th cervical roots
- 5th and 6th roots pass directly through the middle scalene muscle
- Runs under brachial plexus and clavicle then over the 1st rib
- Lateral aspect of chest wall as far down as 8th or 9th rib where it innervates serratus anterior
- Due to the length of the nerve and how superficial it runs, it is more vulnerable to injury
- Traumatic
- Blunt force trauma to thorax or shoulder like during a collision or fall
- Knife wound or other penetrating wound
- Iatrogenic injuries during surgeries
- Non-traumatic
- Entrapment of 5th and 6th cervical nerve roots in middle scalene
- Impingement of nerve between scapula and 2nd rib during traction of the upper extremity
- Compression of the 7th cervical nerve root
- Long Thoracic Nerve impingement under the inferior angle of the scapula during general anesthesia or during passive abduction of the arm
- ***Scapular winging (medial translation of the scapula, inferior angle rotates towards midline, and prominence of the vertebral border, which becomes more prominent with pushing forward against resistance).
- Scapular dyskinesia
- Pain
- Decreased range of motion of shoulder elevation
- Weakness of serratus muscle
Pain referral pattern:
- Around the shoulder
- In antagonist muscles (levator scapulae and both rhomboids)
- Usually caused by spasms due to unopposed muscle contraction because of serratus anterior weakness
- clicking and popping with stressful activities NOT very common
- Severe pain usually due to neuritis, such as Parsonage-Turner Syndrome
Diagnostic tool to rule in/out:
- Physical examination including:
- History
- Signs and symptoms
- Mechanism of injury
- Observation of movements
- Palpation
- Passive/active range of motion
- Manual muscle tests
- Electromyography and nerve conduction tests are used to confirm
- Plain radiographs that could show the presence of cervical spondylosis or a mass lesion, such as scapular osteochondroma, for a patient with scapular winging
- CT and MRI scans are only necessary if there is suspicion of some other type of disease process such as a disc herniation or neoplasm
- In the case that surgical repair is indicated for the long thoracic nerve palsy, the spinal accessory nerve to the trapezius should be included in the nerve conduction test because concomitant trapezius palsy can present complications for the results of the surgery
